![]()
What is the Acromioclavicular (AC) Joint?
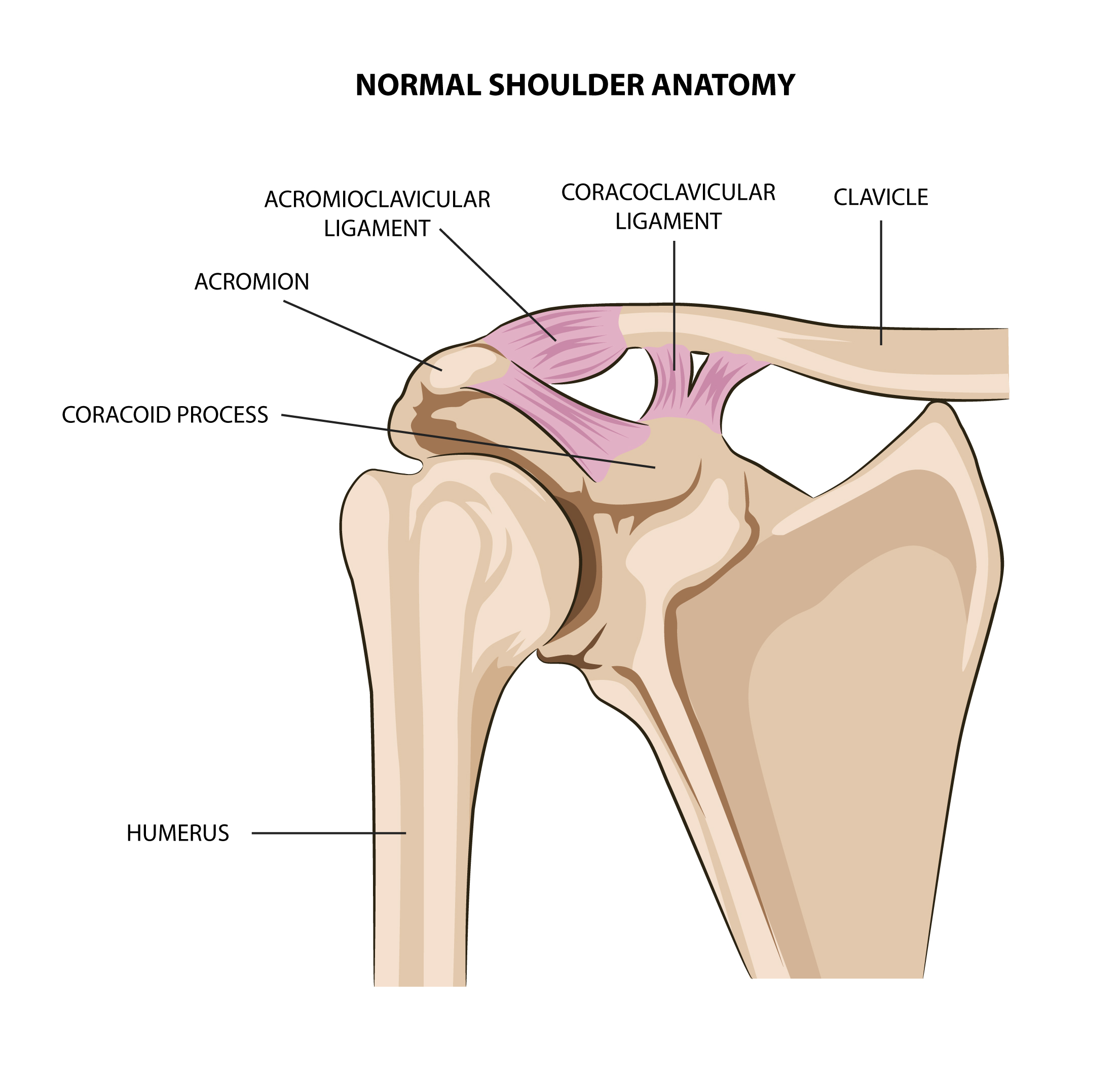
The shoulder girdle is made up of the humerus (armbone), the clavicle (collar bone) and the scapula (shoulder blade). The outer most part of the scapula is called the ‘acromion’, and this joins with the clavicle to form the acromioclavicular (AC) joint. The AC joint is an important part of the shoulder girdle, and helps the shoulder blade achieve more rotation and movement. It also transmits forces from the arm to the clavicle.
At the AC joint the two bones can glide slightly against each other, and are cushioned by a cartilage disc within the joint. The AC joint is supported by strong ligaments that form a capsule around it. Further around the front of the shoulder are other supporting ligaments which connect the clavicle to a projection of bone from the scapula known as the ‘coracoid’. These ligaments are called the ‘coracoclavicular’ ligaments, and help support the AC joint by preventing the clavicle from springing upwards.
What is Acromioclavicular (AC) instability?
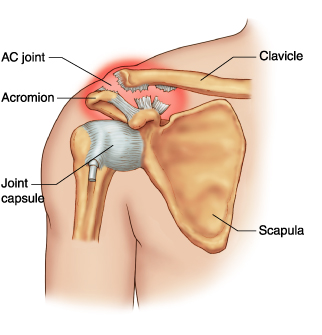
Most commonly occuring as a result of an acute injury, such as a fall from a bike or landing on the shoulder in contact sports, the acromioclavicular joint can become injured and ‘separate’. The ligaments which support the AC joint can get sprained or tear completely. Depending on the pattern of injury and which ligaments are torn, the severity of the injury can range from being mild with minimal pain, to a very unstable joint with severe pain. With more severe injuries there is a noticeable lump over the AC joint as the collarbone becomes more prominent.
What are the symptoms of Acromioclavicular (AC) instability?
An unstable acromioclavicular joint can cause the following symptoms:
- Pain around the front and top of the shoulder
- Deformity and lump at the AC joint, with the clavicle appearing much more prominent
- Weakness and loss of movement of the arm, particularly when bringing the arm overhead and across the body
- Pain when lying on the affected side
How is Acromioclavicular (AC) instability diagnosed?
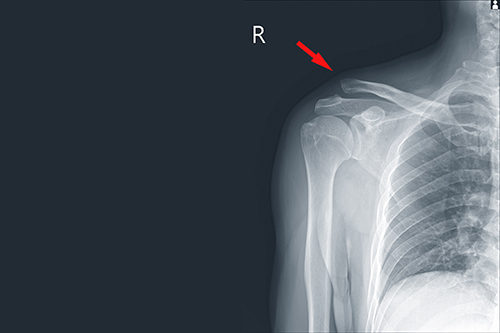
A damaged acromioclavicular joint is usually fairly evident based on the nature of the injury and deformity of the AC joint. The following investigations may be useful:
- X-ray of both shoulders – this is useful to determine the severity of injury, and it can be helpful to compare the injured and uninjured sides.
- MRI – for more chronic acromioclavicular injuries, or to assess the soft tissues around the shoulder, an MRI scan may occasionally be useful.
How is Acromioclavicular (AC) instability treated?
The less severe types of AC joint injuries can be managed non-operatively. This involves the use of a sling for 2-4 weeks before commencing a physiotherapy guided rehabilitation program.
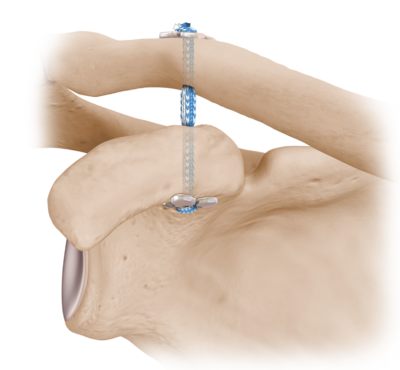
For the higher grade AC joint injuries, a trial of the same non-operative management may be attempted with reasonable results and a return back to sport and work. However, if there is ongoing AC joint pain and instability which impairs sleep, work, sport or other activities, then surgery is recommended. Read more about AC joint stabilisation surgery.
My goals as a surgeon are to relieve your pain, restore your function, and return you back to doing what you love.
– Dr Raymond Yu
- Adelaide Orthopaedic Surgeon
- Adelaide Shoulder Surgeon
About
Dr Raymond Yu
Dr Raymond Yu is an Adelaide Orthopaedic Surgeon with post-Fellowship expertise in Shoulder and Elbow Surgery.
He specialises in orthopaedic surgery of the Shoulder and Upper Limb with a focus on modern keyhole and minimally-invasive techniques.
Dr Yu has a special passion for:
- Rotator cuff repair surgery
- Shoulder replacement surgery
- Shoulder stabilisation surgery
Dr Yu practices at



